Actually, these aren't lessons I learned from Japan as such, but rather lessons learned as a result of living isolated in a foreign culture.
1. Good friends are worth the effort.
Ever had a friend you really really like but don't feel especially close to for whatever reasons are keeping you apart? Maybe they're a long drive away. Maybe they seem to have a lot of other stuff going on in their lives. Maybe you're just not sure how to open up a D&M conversation with them. Or whatever. In these cases, you can expect that your friendship will remain a surface one until one or both of you takes the plunge and makes the effort to get together. Good relationships take time and effort. It can be a risky emotional investment but it's like the financial variety -- high risk, high returns. Closely related to this is:
2. You can't really have a close friendship with someone until you've shared some of the raw, deep and intimately personal experiences of life.
I've had the honour of developing two special friendships during my time in Japan. One of them has been on-line only, nevertheless we now know stuff about each other that either nobody else knows, or at least very few other people know. I consider this woman one of my best friends. The other friend is M, who I've mentioned a few times in passing on this blog. M was very helpful to me in the lead-up to Elliott's birth (poor thing; how could she have ever predicted that she'd meet a crazy Australian who would take her on a grand adventure into the world of freebirthing?), and even more so afterwards when I needed practical support for adjusting to life as mother of two. Later I was able to return the favour in a rather unexpected way; M had a miscarriage, and was able to lean on me for the emotional support she needed to wait out the agonising four weeks between learning that her baby had died and actually having the miscarriage. Her other choice was to have surgery, which she feels she surely would have done, and then regretted, if it hadn't been for my support. After her experience, our friendship took on a palpable new quality, and then when my life fell apart in the last two months of our stay she was there for me in a way I wouldn't have felt comfortable to ask for before. (There's not too many people I'd feel OK to sleep in front of while they watch my kids as well as their own.) Until the last two or three years of my life I've never felt like I had any close friends, but I'm learning to let go of the issues which have historically prevented me from getting close to people, and the result is already so rewarding (see #1).
3. Live church services really are a blessing.
I think this is one of those lessons I already knew in theory, but having lived the reality, I truly understand now. Most of the time on Sabbaths we downloaded sermons off our church's website. Sometimes we were able to hook up to a live church service back home, and we always enjoyed this opportunity to feel a little more involved. But nothing beats actually being there. A human connection is always better than an electronic one. I have a new appreciation of the verse about "not forsaking the assembling of yourselves together" now.
4. It's not better or worse, it's just different.
I must admit that this is one I have to keep reminding myself of, since I left Japan still finding some of its habits kinda irritating, but anyway: So often we can look down on what other cultures do when their practices seem awkward, difficult, inconsistent, gross or just plain weird. Most of the time, though, I think it's just that our comfort zone is being challenged. I started learning this lesson on the very first day we arrived here. We were at Tokyo station and I was busting for a pee. I found some women's toilets and to my mild discomfort realised they were all the squat variety. I had never actually used a squat toilet before, but I was desperate and knew it wasn't worth the effort to go looking for a "Western-style" toilet. So I used it, and it really wasn't that bad. Some weeks later I had to make use of another one and was delighted to discover they're even easier to use when you face the right direction (towards the flush, not away from it). These days squat toilets don't faze me in the slightest. I don't prefer them, but neither do I deliberately avoid them. They're not better or worse, just different. Same deal applies to most things.
Sunday, September 12, 2010
Sunday, July 04, 2010
Izu-Mito Sea Paradise
About three kilometres down the road from Awashima Marine Park is another aquarium and marine park called Izu-Mito Sea Paradise. It's bigger and a little more slick than Awashima; consequently it costs more to get in (1900 yen per adult at the time of writing this) and the dolphins do more entertaining tricks. Unfortunately none of our photos of the fishies turned out very well, but the aquarium is quite extensive and worth a look. Anyway, here's a sample of what's on offer.






Personally I prefer Awashima Marine Park, but this place is still worth a visit if you've got the time. Certainly the dolphin shows here are better, but I think that's the only thing it's got over Awashima.
*****
To get there, take the Kisho bus from stop number 8 on the south side of Numazu Station. It takes roughly half an hour, it's another stop or two past Awashima Marine Park, and it stops on the main road just outside the entrance.

No touristy establishment is complete without the photography service you can pay extra for.

Yep, they're just as ugly up close.

Crush lives here.

I don't know how much extra it costs to don an orange life jacket and see the dolphins jumping from up really close, but I bet it's kind of cool to do so.

The dolphins did some neat tricks with this woman, the most spectacular one being to throw her up really high out of the water (we didn't get it on camera). There's also a show in a different pool featuring seals doing balancing tricks and Pacific white-sided dolphins which swim really fast and do some cool stuff. The interesting thing about that show is that the pool is above ground with a glass wall so you can see what the dolphins are doing under water.

This is less exciting than it looks. But at least it shows you something of what else is there. Other animals include a few varieties of seals, a sea otter and Humboldt penguins (which stink).
Personally I prefer Awashima Marine Park, but this place is still worth a visit if you've got the time. Certainly the dolphin shows here are better, but I think that's the only thing it's got over Awashima.
*****
To get there, take the Kisho bus from stop number 8 on the south side of Numazu Station. It takes roughly half an hour, it's another stop or two past Awashima Marine Park, and it stops on the main road just outside the entrance.
Wednesday, May 26, 2010
Business negotiations, Japanese style
Our air conditioner and hot water system have packed it in, so after a few phone calls back and forth between our caretaker, landlord, the translating company and Daikin Air, I was told a service person would come around this afternoon so could I please stay home. OK, no problem.
At 3:00 this afternoon I get a phone call from Daikin Air. They are very busy today so they can't come until tomorrow. What time would be suitable?
Well we didn't get showers this morning, and Craig didn't have one yesterday either. So really, today would be suitable. But OK, first thing tomorrow would be great.
What time tomorrow morning?
9:00.
Until what time?
Huh? What do you mean until what time, I'll stay here as long as it takes you. How long do you expect it to take?
Maybe one hour.
OK. So 9:00 until 10:00 then. (Although I've caught on to what's really going on now... I'm in the middle of another one of those Japanese cultural experiences.)
And what other times would be suitable?
Bingo, I knew it. Sigh. In the afternoon, 1:00 is fine.
Until when?
Sigh. Any time from 1:00 is fine.
OK then. We will see you at 1:00 tomorrow. Thank you.
Well I'll say this much. At least a service person will show up at 1:00 tomorrow (which would not be guaranteed if this conversation was happening in Australia), and at least they called at 3:00 instead of 5:30. Right. I'm off to the park then.
At 3:00 this afternoon I get a phone call from Daikin Air. They are very busy today so they can't come until tomorrow. What time would be suitable?
Well we didn't get showers this morning, and Craig didn't have one yesterday either. So really, today would be suitable. But OK, first thing tomorrow would be great.
What time tomorrow morning?
9:00.
Until what time?
Huh? What do you mean until what time, I'll stay here as long as it takes you. How long do you expect it to take?
Maybe one hour.
OK. So 9:00 until 10:00 then. (Although I've caught on to what's really going on now... I'm in the middle of another one of those Japanese cultural experiences.)
And what other times would be suitable?
Bingo, I knew it. Sigh. In the afternoon, 1:00 is fine.
Until when?
Sigh. Any time from 1:00 is fine.
OK then. We will see you at 1:00 tomorrow. Thank you.
Well I'll say this much. At least a service person will show up at 1:00 tomorrow (which would not be guaranteed if this conversation was happening in Australia), and at least they called at 3:00 instead of 5:30. Right. I'm off to the park then.
Tuesday, May 18, 2010
In the manner of a river
I recently learned of a beautiful Japanese phrase. Kawa no ji mitai -- "in the manner of a river". The wider context is kawa no ji mitai nemasu, meaning "to sleep in the manner of a river". How on earth does one sleep like a river?
Like this. The kanji for kawa (river) is:
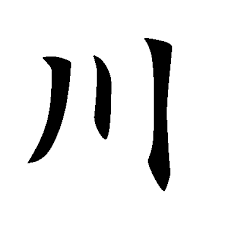 The two outer lines represent the riverbanks and the middle line is the river itself. Sleeping in this manner refers to co-sleeping; the river is the child, the banks are the parents. Isn't that a wonderful image?
The two outer lines represent the riverbanks and the middle line is the river itself. Sleeping in this manner refers to co-sleeping; the river is the child, the banks are the parents. Isn't that a wonderful image?
I learned of this because Craig told me about a conversation he had with one of his work colleagues. They were talking about Elliott, within the context of how often he's waking at night, and it naturally came out that Elliott's in bed with us. Craig's colleague then explained that sleeping with babies is such a common practice in Japan that they even have this phrase for it.
Curious to find out if this was true or just what one person was saying, I did a little googling. I found this article which affirms it. It's a sociology essay comparing American and Japanese infant sleeping practices and how they reflect wider values of their respective cultures. And it mentions kawa:
And then I found this blog post which says pretty much exactly the same thing as the essay, only in a much more readable form. I just think that's cool.
Like this. The kanji for kawa (river) is:
I learned of this because Craig told me about a conversation he had with one of his work colleagues. They were talking about Elliott, within the context of how often he's waking at night, and it naturally came out that Elliott's in bed with us. Craig's colleague then explained that sleeping with babies is such a common practice in Japan that they even have this phrase for it.
Curious to find out if this was true or just what one person was saying, I did a little googling. I found this article which affirms it. It's a sociology essay comparing American and Japanese infant sleeping practices and how they reflect wider values of their respective cultures. And it mentions kawa:
The Japanese... emphasize the value of dependence as the primary socializing experience. The Japanese word for a common cosleeping arrangement demonstrates this value. "The custom of the child sleeping between the parents is referred to as kawa. Kawa is the Japanese character for a river flowing between 2 banks and kawa is therefore used to refer to the child sleeping between the protective support of the 2 parents."
And then I found this blog post which says pretty much exactly the same thing as the essay, only in a much more readable form. I just think that's cool.
Monday, May 10, 2010
A day trip from Numazu to Heda
Heda is a small town on the west coast of the Izu Peninsula. It has a "real" beach, which is its main attraction, and a few other features to keep the tourists coming. A small onsen, a smattering of temples, giant crabs, a museum of... something which I forget now.
We just spent the day walking around. The first hour was spent wandering the streets, stopping to check out the outside of the onsen (boring) and watch a mother and two kids feeding koi (those gigantic goldfish) in one of the local canals. Then we walked all around the bay to the beach area and spent the rest of our time hanging around there, and walking around the head of the bay too.
Heda is an isolated place that's apparently quite difficult to get to. It's only 28km from Numazu by road, but it's a very narrow and winding road so it'll take you at least an hour and probably longer if you get stuck behind someone slow. (Apparently it takes five hours to get to from Tokyo in the peak of summer.) We went by ferry; the "White Marine" departs from the northwest end of the Numazu port, takes half an hour and costs 2000 yen one-way. So it's pricey, but has some novelty value and quite spectacular scenery along the way.





***** ***** *****
The ferry timetable is hard to find on the internet; even harder to find in English. Your best bet is probably to just head down to the ticket office at the port (the room at the end of the dinky little building across and up the road a bit from the Fishmarket Taproom and Baird Brewery), or you could probably ask at the Taproom itself, since everybody speaks English there. We took the 9:00 a.m. ferry; the next one was at 11:00 a.m., but that was the timetable for spring and summer. It varies throughout the year. Going back, we took the last ferry at 3:15 p.m.
We just spent the day walking around. The first hour was spent wandering the streets, stopping to check out the outside of the onsen (boring) and watch a mother and two kids feeding koi (those gigantic goldfish) in one of the local canals. Then we walked all around the bay to the beach area and spent the rest of our time hanging around there, and walking around the head of the bay too.
Heda is an isolated place that's apparently quite difficult to get to. It's only 28km from Numazu by road, but it's a very narrow and winding road so it'll take you at least an hour and probably longer if you get stuck behind someone slow. (Apparently it takes five hours to get to from Tokyo in the peak of summer.) We went by ferry; the "White Marine" departs from the northwest end of the Numazu port, takes half an hour and costs 2000 yen one-way. So it's pricey, but has some novelty value and quite spectacular scenery along the way.

Don't ask me how those people got to those rocks, but I think they were still there on our way back in the afternoon.

This beach gets packed out with people in summer. If it had been a clear day, you'd be able to see Mt Fuji in the background of this photo.

Cos she's a cutie.


Cos the pictures amuse me.
***** ***** *****
The ferry timetable is hard to find on the internet; even harder to find in English. Your best bet is probably to just head down to the ticket office at the port (the room at the end of the dinky little building across and up the road a bit from the Fishmarket Taproom and Baird Brewery), or you could probably ask at the Taproom itself, since everybody speaks English there. We took the 9:00 a.m. ferry; the next one was at 11:00 a.m., but that was the timetable for spring and summer. It varies throughout the year. Going back, we took the last ferry at 3:15 p.m.
Tuesday, April 27, 2010
You haven't really LIVED in Japan until...
You've sat naked in a hot tub with some random strangers.
Yep, I went to a real onsen today. By choice -- sort of. My friend M suggested we go and I thought well hey, when we move home am I going to be able to look back on our time here and say yeah I did do some pretty interesting things, or not? So I took a deep breath and chanted "this is culturally normal, this is culturally normal, this is culturally normal" to myself, and even managed to act like I was perfectly fine with it.
And actually, I even enjoyed the experience. Not so much the naked bit per se, but standing in a room with women of all ages, shapes and sizes who were simply enjoying life and not being hung up over whether their thighs are too fat or their boobs are too small or the mole on their back is too big. There's something beautiful about four women in their seventies sitting naked in a hot tub, laughing together over some private joke, smiling and asking you in Japanese how old your kawaii little baby is.
Tell ya what though, it was a good reminder of the reality that one day I'm gonna get old and saggy. Everywhere.
Yep, I went to a real onsen today. By choice -- sort of. My friend M suggested we go and I thought well hey, when we move home am I going to be able to look back on our time here and say yeah I did do some pretty interesting things, or not? So I took a deep breath and chanted "this is culturally normal, this is culturally normal, this is culturally normal" to myself, and even managed to act like I was perfectly fine with it.
And actually, I even enjoyed the experience. Not so much the naked bit per se, but standing in a room with women of all ages, shapes and sizes who were simply enjoying life and not being hung up over whether their thighs are too fat or their boobs are too small or the mole on their back is too big. There's something beautiful about four women in their seventies sitting naked in a hot tub, laughing together over some private joke, smiling and asking you in Japanese how old your kawaii little baby is.
Tell ya what though, it was a good reminder of the reality that one day I'm gonna get old and saggy. Everywhere.
Wednesday, February 24, 2010
Homebirth options in Japan
This post is written for anyone researching homebirth and/or freebirth in Japan. Please note that I am speaking of my personal experience only, and make no claims that because it happened this way for me it will be the same for others. However, I am sharing my experience so that anyone interested can see what's possible for themselves.
The focus of this post is freebirth, also known as unassisted birth. I wasn't very interested in having a Japanese homebirth midwife for a couple of reasons which I will explain in a moment, although I did briefly investigate this option. As it was impractical for me to go back to Australia for the birth, I also attempted to find an Australian midwife willing to come over to Japan to attend me. However, my efforts were unsuccessful, so freebirth was it. I did have a doula in attendance, who came over from Australia. (As far as I can tell, doulas do not exist in Japan.)
The reasons I chose not to have a Japanese homebirth midwife are: 1) I wanted an attendant who could speak fluent English, because communication difficulties were not something I was prepared to put up with while in labour. Very few Japanese midwives speak English, let alone fluently. 2) Homebirth midwives in Japan are not independent practitioners, which means they are required to have a back-up doctor and hospital, and are therefore bound by that doctor and hospital's birth policies. This means that the pregnant woman is obligated to pass a whole lot of tests and submit to a whole lot of antenatal appointments and procedures in order to be considered "low-risk" enough to give birth at home. I am opposed to the routine use of medical procedures and tests during pregnancy and birth, which is why I knew having a Japanese midwife was not in my best interests.
Another factor I needed to consider was that I wanted to have a waterbirth. Waterbirths are not available in Japanese hospitals. Women who choose homebirth with a midwife in Japan may be able to have a waterbirth if the midwife is comfortable with the idea (not all of them are) and they are willing to organise a birth pool for themselves. Most women who take this option simply use their bath. This wasn't possible for me, because our bath wasn't large enough. I ended up borrowing a La Bassine "Made in Water" birth pool from a friend back in Australia, and we set it up in our lounge room with a hose running from the kitchen tap to fill it.
An important thing to know that freebirth is legal in Japan. It's rare -- I know of only one other planned freebirth to have occurred here, and even in that case it's only hearsay, I have not been in direct contact with the couple involved. But just because it doesn't happen very often, doesn't mean it's not an option, either from a legal or practical standpoint.
Of course, any intelligent freebirther is going to take careful steps to ensure she has an appropriate back-up plan in case transfer to hospital during or after birth becomes necessary. In most cases, calling the emergency ambulance number (119) is sufficient. You don't actually need a back-up booking at a hospital, because when you call for an ambulance they will just send you to the nearest available hospital.
For the administrative side of things, the documents required are:
* The boshi techo, or mother and child health handbook.
Strictly speaking this is actually not necessary, however it makes things run a lot more smoothly if you do have it. Ordinarily you collect a boshi techo from your local city health centre after receiving a pregnancy confirmation certificate from your doctor. Since I was having an unassisted pregnancy, I didn't have a doctor or pregnancy confirmation certificate, so I didn't collect a boshi techo until week 34 of my pregnancy by which time it was extremely obvious that I was pregnant. (Anecdotally, I know someone who turned up to her city health centre at 8 weeks pregnant and told them she was still looking for a midwife, and that was good enough for them.)
* The shussei shomeisho
* The shussei todoke
It's a dog's breakfast trying to understand what these documents are if you google them. Every single website seems to have a different (often contradictory) explanation of what they actually are, and what the difference is between them, etc. I still don't get it either. All I know is that they're required for registering your baby's birth, and are equivalent to a birth certificate. To add to the confusion, some websites refer to a single document called the shussei todoke juri shomeisho or shussei todoke kisaijiko shomeisho. So all I'm going to do is explain what I did to get hold of them:
I went to the city office at 34 weeks with a Japanese friend who explained to the staff that I was freebirthing but would have a doula in attendance, and that I needed a copy of the shussei shomeisho. They handed over the document, which was actually the shussei todoke and shussei shomeisho together on an A3-sized sheet of paper, with no questions asked. I'm not sure if I was just plain lucky and got an open-minded staff member that day, if having a Japanese friend with me helped, or if it was of no concern to the city office what kind of birth I was planning anyway. My friend was pleasantly surprised that it was as simple as that to get hold of the form, because it is ordinarily issued by the hospital you give birth in. In any case, the important thing is that the shussei shomeisho has provision on it for someone other than a doctor or midwife to sign that they witnessed the birth. This made registering my baby's birth a piece of cake since I had a doula who signed it for me. I'm not sure what you would do if you go totally unassisted, or just have your partner there. I was told by a nurse early on in my pregnancy that the form had to be signed by someone other than the baby's parents (although it would certainly be worth verifying this for yourself if that's the option you wish to take, because one thing I learned through this whole experience was "don't just take a nurse or doctor's word for it").
The shussei shomeisho needs to be lodged in person at the city office within 14 days of the birth. They wave their magic wand over it and hand it back to you in the form of a stamped photocopy (there's a small fee involved). That document becomes your all-important shussei todoke, or birth certificate. You might want to consider obtaining more than one copy of it. Fortunately if you ever need another one, you can just rock up to your city office and they'll give you a copy for another small fee.
After the registration process is done, all other documents you need (alien registration card, visas, re-entry permits, registration with your own country, passports, etc) are processed exactly the same way they'd be processed if your baby was born in hospital, and information on how to go about organising all of that is readily available via your city office and embassy or consulate.
If you have any questions, please contact me by leaving a comment here.
The focus of this post is freebirth, also known as unassisted birth. I wasn't very interested in having a Japanese homebirth midwife for a couple of reasons which I will explain in a moment, although I did briefly investigate this option. As it was impractical for me to go back to Australia for the birth, I also attempted to find an Australian midwife willing to come over to Japan to attend me. However, my efforts were unsuccessful, so freebirth was it. I did have a doula in attendance, who came over from Australia. (As far as I can tell, doulas do not exist in Japan.)
The reasons I chose not to have a Japanese homebirth midwife are: 1) I wanted an attendant who could speak fluent English, because communication difficulties were not something I was prepared to put up with while in labour. Very few Japanese midwives speak English, let alone fluently. 2) Homebirth midwives in Japan are not independent practitioners, which means they are required to have a back-up doctor and hospital, and are therefore bound by that doctor and hospital's birth policies. This means that the pregnant woman is obligated to pass a whole lot of tests and submit to a whole lot of antenatal appointments and procedures in order to be considered "low-risk" enough to give birth at home. I am opposed to the routine use of medical procedures and tests during pregnancy and birth, which is why I knew having a Japanese midwife was not in my best interests.
Another factor I needed to consider was that I wanted to have a waterbirth. Waterbirths are not available in Japanese hospitals. Women who choose homebirth with a midwife in Japan may be able to have a waterbirth if the midwife is comfortable with the idea (not all of them are) and they are willing to organise a birth pool for themselves. Most women who take this option simply use their bath. This wasn't possible for me, because our bath wasn't large enough. I ended up borrowing a La Bassine "Made in Water" birth pool from a friend back in Australia, and we set it up in our lounge room with a hose running from the kitchen tap to fill it.
An important thing to know that freebirth is legal in Japan. It's rare -- I know of only one other planned freebirth to have occurred here, and even in that case it's only hearsay, I have not been in direct contact with the couple involved. But just because it doesn't happen very often, doesn't mean it's not an option, either from a legal or practical standpoint.
Of course, any intelligent freebirther is going to take careful steps to ensure she has an appropriate back-up plan in case transfer to hospital during or after birth becomes necessary. In most cases, calling the emergency ambulance number (119) is sufficient. You don't actually need a back-up booking at a hospital, because when you call for an ambulance they will just send you to the nearest available hospital.
For the administrative side of things, the documents required are:
* The boshi techo, or mother and child health handbook.
Strictly speaking this is actually not necessary, however it makes things run a lot more smoothly if you do have it. Ordinarily you collect a boshi techo from your local city health centre after receiving a pregnancy confirmation certificate from your doctor. Since I was having an unassisted pregnancy, I didn't have a doctor or pregnancy confirmation certificate, so I didn't collect a boshi techo until week 34 of my pregnancy by which time it was extremely obvious that I was pregnant. (Anecdotally, I know someone who turned up to her city health centre at 8 weeks pregnant and told them she was still looking for a midwife, and that was good enough for them.)
* The shussei shomeisho
* The shussei todoke
It's a dog's breakfast trying to understand what these documents are if you google them. Every single website seems to have a different (often contradictory) explanation of what they actually are, and what the difference is between them, etc. I still don't get it either. All I know is that they're required for registering your baby's birth, and are equivalent to a birth certificate. To add to the confusion, some websites refer to a single document called the shussei todoke juri shomeisho or shussei todoke kisaijiko shomeisho. So all I'm going to do is explain what I did to get hold of them:
I went to the city office at 34 weeks with a Japanese friend who explained to the staff that I was freebirthing but would have a doula in attendance, and that I needed a copy of the shussei shomeisho. They handed over the document, which was actually the shussei todoke and shussei shomeisho together on an A3-sized sheet of paper, with no questions asked. I'm not sure if I was just plain lucky and got an open-minded staff member that day, if having a Japanese friend with me helped, or if it was of no concern to the city office what kind of birth I was planning anyway. My friend was pleasantly surprised that it was as simple as that to get hold of the form, because it is ordinarily issued by the hospital you give birth in. In any case, the important thing is that the shussei shomeisho has provision on it for someone other than a doctor or midwife to sign that they witnessed the birth. This made registering my baby's birth a piece of cake since I had a doula who signed it for me. I'm not sure what you would do if you go totally unassisted, or just have your partner there. I was told by a nurse early on in my pregnancy that the form had to be signed by someone other than the baby's parents (although it would certainly be worth verifying this for yourself if that's the option you wish to take, because one thing I learned through this whole experience was "don't just take a nurse or doctor's word for it").
The shussei shomeisho needs to be lodged in person at the city office within 14 days of the birth. They wave their magic wand over it and hand it back to you in the form of a stamped photocopy (there's a small fee involved). That document becomes your all-important shussei todoke, or birth certificate. You might want to consider obtaining more than one copy of it. Fortunately if you ever need another one, you can just rock up to your city office and they'll give you a copy for another small fee.
After the registration process is done, all other documents you need (alien registration card, visas, re-entry permits, registration with your own country, passports, etc) are processed exactly the same way they'd be processed if your baby was born in hospital, and information on how to go about organising all of that is readily available via your city office and embassy or consulate.
If you have any questions, please contact me by leaving a comment here.
Subscribe to:
Posts (Atom)